
Anterior Cruciate Ligament Reconstruction
What is the Anterior Cruciate Ligament (ACL)?
The Anterior Cruciate Ligament (ACL) is one of the major stabilising ligaments in the knee. It is a strong rope-like structure located in the centre of the knee, running from the femur to the tibia.
What Does the ACL Do?
The ACL prevents the tibia (shin bone) from moving abnormally on the femur (thigh bone). When this abnormal knee movement occurs, it is referred to as knee instability, and the patient is aware of it.
Often, other structures such as the meniscus, the articular cartilage (lining the joint) or other ligaments can also be damaged simultaneously as a cruciate injury. These may need to be addressed at the time of surgery.
- Most injuries are sports-related, involving a twisting injury to the knee.
- It can occur with a sudden change of direction, a direct blow, e.g., a tackle, landing awkwardly.
- Often, there is a popping sound when the ligament ruptures.
- Swelling usually occurs within hours.
- There is often the feeling of the knee popping out of the joint.
- It is rare to be able to continue playing sports with the initial injury.
What is ACL Reconstruction?
ACL reconstruction remains the most reliable way of restoring knee stability in athletes who have knee instability following ACL rupture. ACL reconstruction is a surgical procedure that aims to replace a torn ACL with a new ligament. The new ligament is typically taken from other parts of the patient's body or a donor. This surgery can now be performed with minimal incisions and low complication rates. Physiotherapy is important in recovery.
Who is Suitable for ACL Reconstruction?
If you have experienced an ACL tear or damage, and your symptoms have not improved with non-surgical treatments, you may be a good candidate for ACL Reconstruction. You may also be suitable for this procedure if you have a highly active lifestyle or participate in sports requiring sudden direction or pivoting changes. After a thorough evaluation and diagnostic testing, an orthopaedic surgeon can determine if ACL Reconstruction is the best option for you.
Benefits of ACL Reconstruction
There are several benefits of ACL reconstruction. First, it can help restore knee stability and function, allowing you to resume daily activities or sports without pain or discomfort. Second, it can reduce the risk of long-term complications such as arthritis or meniscal tears. Third, it can improve your quality of life and overall well-being by reducing the risk of further knee injuries and the need for future surgical interventions.
ACL Reconstruction vs ACL Repair
Repair involves keeping the original ligament by directly suturing the two ends of the rupture together. Attempts at repair of ACL tears are now largely historical due to the high rate of failure of the surgery.
All ACL surgery nowadays is a reconstruction. This involves replacing the damaged tissue with a substitute tissue called a graft. The most commonly used grafts involve tissue from the patient (autografts). Tissue from donor patients (allografts) can also be used, as can synthetic ligaments.
Types of ACL Reconstruction
- Autograft Ligaments
- Cadaver Ligaments
- Synthetic Ligaments
Autograft Ligaments
The most commonly used autografts are
- Hamstring tendons
- Patella ligament
- Quadriceps tendons
There are pros and cons for each option. All three options are suitable and are associated with good results.
Cadaver Ligament
There are pros and cons of using cadaver tendons.
Pros
- Readily available
- Less painful operation with quicker recovery (because your tissue is not harvested)
Cons
- Tiny risk of infection
- Takes longer for the graft to incorporate
- Has a higher failure rate than using your own tissue
Synthetic Ligament
Synthetic ligaments are not new technology. They were used more than 20 years ago. Despite the initial good early results, they fell out of favour because the longer-term results were not as good. Popularity was resurgent in using synthetic ligaments more recently, but this has again fallen from favour.
Preoperative Preparation for ACL Reconstruction
Before undergoing ACL reconstruction surgery, you should undergo several tests to assess the extent of the injury and determine the best course of treatment. These tests include a physical examination, X-rays, MRIs, and blood tests. Your surgeon will also review your medical history and provide pre-operative instructions, such as avoiding food and drink for a certain period before the surgery.
ACL Reconstruction Procedure
Surgery is performed as a day procedure or an overnight stay.
The surgery usually takes between 60–90 minutes.
Surgical techniques have improved significantly over the last decade, complications are reduced, and recovery is much quicker than in the past.
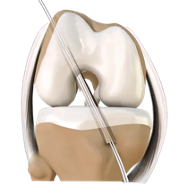
The surgery is performed arthroscopically.
- The ruptured ligament is removed, and tunnels (holes) in the bone are drilled to accept the new graft.
- This graft, which replaces your old ACL, is taken either from the hamstring tendon (or an artificial ligament is used). Your doctor will discuss these options with you before surgery.
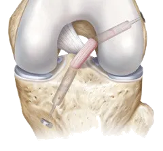
- The graft is prepared to take the form of a new tendon and passed through the drill holes in the bone.
- The new tendon is then fixed into the bone with various devices to hold it while the ligament heals into the bone (usually six months).
- The rest of the knee can be visualised simultaneously, and any other damage is dealt with, e.g. meniscal tears.
- The wounds are then closed, and a dressing is applied.
Post-operative Recovery for ACL Reconstruction
Pain Management
You will have pain medication by tablet or in a drip (intravenous).
Wound Care
Leave any waterproof dressings on your knee until your post-op review.
- You can put all your weight on your leg.
- Put ice on the knee for 20 minutes, as frequently as possible.
Post-op review
The first review will usually be after 10-14 days.
Physiotherapy
You will be seen by a physiotherapist who will teach you to use crutches and show you some simple exercises at home.
Exercise and therapy can begin after a few days or be arranged at your first post-op visit.
Why is Rehabilitation for ACL Reconstruction Essential?
Physiotherapy is integral to the treatment and should start as early as possible. Pre-operative physiotherapy helps prepare the knee for surgery better. The early aim is to regain range of motion, reduce swelling and achieve full weight-bearing.
A physiotherapist will supervise your progress and provide a graduated exercise program to prepare you for maximal recovery.. Cycling can begin at six weeks ; jogging generally starts at around three to four months. The graft is strong enough to allow sport at about six to nine months, depending on the activity. However, other factors come into play, such as confidence, fitness and adequate training.
Professional athletes often return at six months, but recreational athletes may take 10 -12 months, depending on motivation and time put into rehabilitation.
Associating injuries to the knee, such as damage to the meniscus, articular cartilage, or other ligaments, can affect the rehabilitation and overall success of the procedure.
ACL Reconstruction Risks & Complications
Like any surgery, anterior cruciate ligament reconstruction has risks. Some of the potential complications include
- Infection,
- Blood clots,
- Nerve damage,
- Graft failure,
- Knee stiffness,
- Chronic pain.
The risk of complications is generally low, and most patients experience a successful outcome. However, it is essential to discuss the risks and benefits of the surgery with an orthopaedic surgeon before deciding to undergo the procedure.
ACL Reconstruction Prognosis
The prognosis of ACL reconstruction is generally good, with a success rate of around 90%. Most patients experience significant improvement in knee function and return to their regular activities or sports within six to twelve months after surgery. However, the success rate depends on various factors, such as the extent of the injury, the age and activity level of the patient, and adherence to post-operative rehabilitation protocols.


