
Knee Osteotomy
What is a Knee Osteotomy?
Knee osteotomy is a surgical procedure designed to shift the weight-bearing load from a damaged or arthritic part of the knee to a healthier area. This is done by cutting and reshaping the bones surrounding the knee joint.
Most osteotomies for knee arthritis are done on the tibia (shinbone) to correct a bowlegged alignment that puts too much stress on the knee's inner (medial) compartment.
The procedure preserves damaged joint tissue, and this surgery can delay or prevent the need for a
Partial or
Total Knee Replacement.

Who is Suitable for Knee Osteotomy?
Knee osteotomy is typically recommended for people who are young, active, and have early-stage arthritis that only affects one part of the knee joint. Candidates for knee osteotomy should also have good knee alignment, be of average weight, and have no significant ligament damage.
Benefits of Knee Osteotomy
Knee osteotomy offers a range of benefits to patients, including
- Joint Preservation: The primary benefit of knee osteotomy is that it helps preserve the natural knee joint by delaying the need for more invasive procedures like total knee replacement.
- Pain relief: Knee osteotomy can relieve pain caused by knee arthritis, allowing patients to resume activities they enjoy.
- Delaying Total Knee Replacement: For younger patients who are not suitable candidates for knee replacement due to their age, osteotomy can provide relief and extend the life of their natural knee joint.
- Improved function: Knee osteotomy can improve knee function, enabling patients to perform activities of daily living more comfortably.
- Quick recovery: Recovery from knee osteotomy is typically faster than knee replacement surgery, with most patients returning to normal activities within six months.
Types of Knee Osteotomy
There are several types of knee osteotomy, including
- High Tibial Osteotomy: This is the most common type of knee osteotomy, which involves cutting and reshaping the upper part of the shinbone to shift the weight-bearing load away from the damaged part of the knee.
- Tibial Tubercle Osteotomy: This type of osteotomy is less common and is typically performed in conjunction with other knee procedures. It involves cutting and repositioning the bony bump at the top of the shinbone to improve knee alignment.
High Tibial Osteotomy
What is a High Tibial Osteotomy?
A High Tibial Osteotomy (HTO) is a surgical procedure that involves cutting and repositioning the upper part of the tibia (the shinbone) to relieve pain and improve function in patients with knee osteoarthritis or other conditions that cause knee joint misalignment.
An HTO aims to shift the weight-bearing load away from the damaged part of the knee joint, typically the inner (medial) side, to the healthy side. Doing so reduces the pressure on the damaged part, and the joint can heal and function more effectively.
Who is Suitable for High Tibial Osteotomy?
High Tibial Osteotomy is commonly indicated for patients with osteoarthritis that is isolated to a single compartment (unicompartmental osteoarthritis) who are too young to consider undergoing Knee Replacement Surgery.
High Tibial Osteotomy is usually performed in arthritic conditions affecting only one side of your knee. The aim is to take pressure off the damaged area and shift it to the other side of your knee with healthy cartilage.
The most common scenario is a patient with a bowed leg because the knee's inner (medial) part has arthritis and is worn away.
How is HTO Suitability Determined?
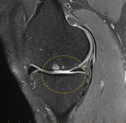
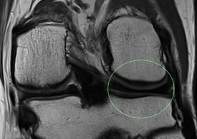
You will require an MRI scan of your knee to investigate suitability for surgery. This ensures other critical parts of your knee are also not damaged by arthritis.
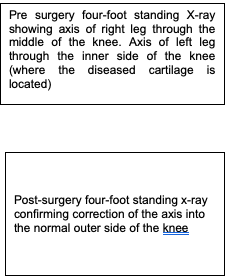
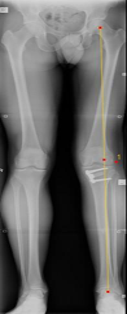
Long X-ray Required
A special long X-ray is taken while standing from your pelvis to your ankles. This x-ray helps calculate where most of the load is distributed in your knee, the severity of the deformity affecting the knee, and the degree of correction required to unload the diseased part of the knee.
High Tibial Osteotomy Procedure
High Tibial Osteotomy is a major surgical procedure; on average, the surgery lasts 2 hours.
- You will require a general anaesthetic. Your doctor utilises Computer Navigation during the surgery to increase the accuracy.
- The initial part of the surgery involves inspecting the inside of the knee with a telescope (Arthroscopy).
- The Computer Navigation requires special sensors to be attached to the thigh bone and shinbone via pins. These pins are removed after the surgery.
- Before the osteotomy is performed, the computer calculates the alignment of the leg utilising the sensors attached to the bone.
- The upper part of the shinbone (tibia) is then carefully dissected, and temporary wires are inserted under X-ray guidance into the bone along the lines of the proposed osteotomy.
- The osteotomy is then performed using a saw. The osteotomy is then opened up, and the computer calculates the correction in real time until the predetermined correction amount is achieved.

- A special plate and screws are then used to hold the osteotomy in position.
- During the surgery, your doctor will usually add a wedge of bone depending on the site of arthritic damage. These blocks of bone are taken from the top of your pelvis and packed into the osteotomy site to promote accelerated healing.

Recovery After High Tibial Osteotomy
Will I Need To Wear A Brace?
Yes, you will need a brace for 12 weeks following your surgery. The brace will initially only allow the knee to fully straighten and allow 30 degrees of bend for the first two weeks while your wounds heal.
From weeks 2 to 8 post-surgery, your brace will be progressively unlocked to allow more bending.
Can I Put Weight On My Leg?
For six weeks after surgery, you can only rest your leg on the ground for balance (touch weight bearing).
For the next six weeks, you will be able to progressively put more weight through your leg until it is fully weight-bearing at the 12-week mark post-surgery.
How Long Does It Take To Make A Full Recovery?
The bone will take 12 weeks to heal, but the full recovery will take 9-12 months due to the rehabilitation required.
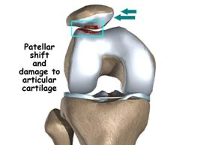
What is a Tibial Tubercle Osteotomy?
Tibial Tubercle Osteotomy (TTO) is a surgical procedure to improve the alignment of the patella. This is performed by changing the insertion point of the patellar tendon on the tibia (tibial tubercle).
How is the Surgery Performed?
You will be admitted to the hospital on the day of your surgery.
Your surgery will be performed using either a general anaesthetic or a spinal anaesthetic, depending on your and your surgeon’s preference.
The initial part of the procedure involves inserting a telescope (called an arthroscope) into the knee joint and inspecting it for damage to the articular cartilage surfaces.
At this stage, any cartilage injuries can be treated.
A 9-14 cm incision is then made on the front part of the knee. A 6 cm long bony segment of the patellar ligament attachment (called the tibial tubercle) is repositioned and held in position with two screws to heal in this new location.
The TTO is performed to move the attachment to the inner side (medial) or further down the tibia (distal). A surgical drain is often used and then removed within the first 24 hours. The surgical incision is usually closed with dissolvable sutures.
Frequently Asked Questions
How will my pain be controlled after surgery?
A local anaesthetic around the knee will decrease your pain during surgery. The anaesthetist often injects an additional anaesthetic called a nerve block while you are asleep. This has a significant impact on reducing the amount of pain you experience.
In addition, you will be given long-acting analgesic tablets to reduce your pain. You will be sent home from the hospital with a prescription for oral pain medication. The most commonly prescribed medications include anti-inflammatories (e.g. Celebrex), regular panadol and breakthrough pain medication (e.g. Endone).
Following week three, you will decrease your pain medication use before physiotherapy and bedtime. Most patients will not require any pain medication past six weeks.
When will I follow up with my surgeon after surgery?
Your first postoperative visit will be with your surgeon in 2 weeks. This appointment is critical for checking your incision healing and range of motion and answering any questions.
You will then follow- up with your surgeon
- six weeks after surgery,
- 12 weeks after surgery,
- 6 months after surgery, and
- one year after surgery.
X-rays will be ordered at each visit until the 3-month mark to ensure the TTO is healing. You will discuss your return to higher-level activity at one year post-op with your surgeon. After your first year, you will follow up with your surgeon yearly.
Do the screws need to be removed in the future?
Some patients do find irritation from the retained hardware; in these cases, both screws can be removed during a day surgical arthroscopy.
When will I start physiotherapy?
You will start physiotherapy in the hospital on the day after surgery, which will continue once you are discharged. You will need to see your physiotherapist generally twice a week for the first six weeks, once a week for the next six weeks, and then reduce the visits from this time.
What will I do during physiotherapy?
The primary goal of physiotherapy is to initially increase ROM so that you do not get stiff following surgery. You will then begin to work on increasing strength and balance after surgery. You will receive a detailed protocol for what you should and should not do during each postoperative phase. You will provide this to your physiotherapist.
When do I need to wear my brace?
You must wear your brace anytime you move around on your crutches. You will use your brace for 6-8 weeks on average.
How long will I need to use my crutches?
Depending on how quickly your bone heals and your surgeon’s preference, you must use your crutches for an average of 6 to 8 weeks.
When can I drive?
For patients undergoing right leg surgery, you may not return to driving until you have discontinued using your crutches (approximately six weeks). For patients undergoing left knee surgery that does not drive manual vehicles, you may return to driving between 3 and 6 weeks when you are no longer taking pain medication.
When can I shower?
You may shower following surgery with your knee brace off, but you must be sitting down at all times. Water-proof bandages will cover your incision. It is advisable to have someone help you get dry and dressed. The knee brace must then be re-applied.
When can I go back to work?
This will be different for each patient and depends mainly on the type of work you do. Most patients working in a sedentary position or desk work will return to work in 4-6 weeks. Patients in more labour-intensive jobs may be out of work for up to 12 weeks.
When can I resume my regular activity?
Return to normal activity depends highly on each patient’s definition of everyday activity. Non-impact activities such as walking, swimming, bike riding, and elliptical training can all be resumed in 3-4 months. Higher-demand activities such as running and sports cannot be resumed until at least 8-12 months.
Knee Osteotomy Prognosis
In general, knee osteotomy has a high success rate, with many patients experiencing significant pain relief and improved knee function. However, it may not suit everyone, and some patients may require additional surgery or alternative treatments.
Knee Osteotomy Risks
Like any surgical procedure, knee osteotomy carries some risks, including infection, bleeding, nerve damage, and blood clots. Other potential risks include failure of the bone to heal correctly, loss of range of motion, and persistent pain or swelling. Your orthopaedic surgeon will discuss these risks with you before the procedure and take steps to minimise the risk of complications.
What if Knee Osteotomy is Delayed?
If knee osteotomy is delayed, the condition causing knee pain may worsen, leading to more significant damage to the knee joint and increased pain and disability. In some cases, delaying knee osteotomy may result in the need for more extensive surgery, such as knee replacement surgery, which is a more invasive and complex procedure.


